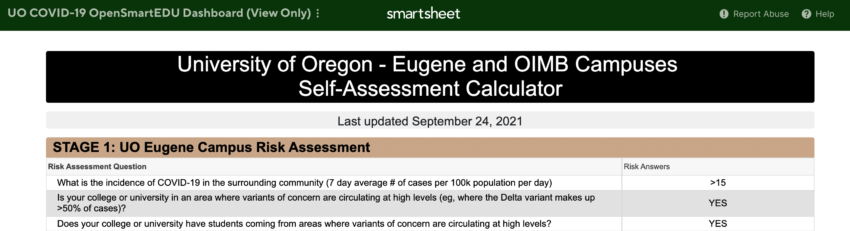
And thanks to an anon reader for finding where that “very low” comes from: a spreadsheet that looks at delta cases, and despite the “this Dashboard is updated every Monday” claim hasn’t been updated since September:
And thanks to an anon reader for finding where that “very low” comes from: a spreadsheet that looks at delta cases, and despite the “this Dashboard is updated every Monday” claim hasn’t been updated since September:
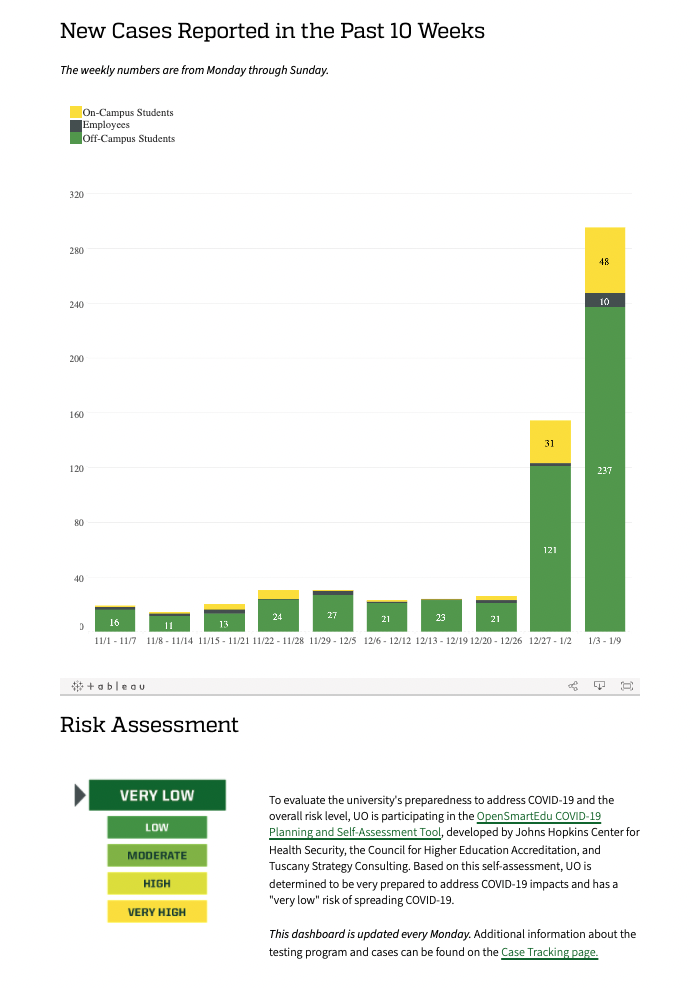
The last bar is labeled “1/3 – 1/9” but today is only 1/6. I’m guessing the data are through 1/5 at most. So it already looks like a big spike and we are missing more than half of the reporting period. Yikes.
Sort of makes you wish we still had a medical school.
Cases are also likely being massively underreported as many students, particularly off-campus, simply aren’t getting tested. I’d like to see yesterday and today’s numbers too. All classes should be pushed online for a couple weeks during this surge, but
I do agree with the sentiment most spread is happening at gatherings, bars, etc. Still, many students don’t feel safe going to classes, big or small, and it’s not sustainable to have so many absences.
Very low, but not as low as the chances that we’ll see an increase that matches this year’s likely inflation, plus make-good for last year’s freeze. (A real raise would be nice as well, but I dare not even dream of that.)
I’d clock that at something like a 10% nominal increase, if commenced immediately. I’m sure an economist could guess better.
The risk assessment form was last updated September 24, 2021: https://app.smartsheet.com/b/publish?EQBCT=929a5f77ce174202930cb5ee96c7dbdd
That is hilarious. Disturbing, but hilarious. That said I’m sure our President and Provost’s decisions have been guided by careful assessment and consideration of the risk tradeoffs … oh fuck it, lets all go bowling and get the omicron over with.
” lets all go bowling and get the omicron over with.”
Let’s not. As we all should know by now, “mild” cases range from “no worse than a cold” all the way to “worst illness I’ve ever been through but I didn’t need the ICU to stay alive.”
Not to mention approximately a third or so of ALL cases develop long-term or permanent physical damage. Speaking as someone who already has a chronic illness and nerve damage… y’all DO NOT WANT.
Please, for the love of Betty White, do everything you can to avoid spreading this virus. (Side benefit: you’ll avoid all the other airborne/aerosol viruses too! Rhinovirus, influenza, tuberculosis, MERS, freaking chickenpox!)
I certainly know of several people (both faculty and students) out with COVID, who haven’t reported to the university.
Didn’t everyone but the administration see this coming? At this point when they say, “Campus will definitely stay open! Absolutely no need to close anything!”, I think, “Yeah, you’ve been so right in all your planning so far…”
From a health perspective among the UO population is this riskier than the H1N1 pandemic of 2009 at this point with Omicron?
dude, were 1300 people a day dying of H1N1? I don’t remember that.
1300 people aren’t dying every day from Omicron (yet).
Also, we didn’t do mass surveillance testing of H1N1 back then like we do for Covid, particularly in nursing homes which still account for a large fraction of deaths.
I do know two fairly young people who were hospitalized from H1N1 in 2009 (which is more than Covid to date, and definitely Omicron). The only people I know who were hospitalized with Covid were older people pre vaccination with several comorbidities.
I like that “yet.” hmmm, somehow ICU’s were not filling up all over the country with H1N1 patients or anything like that. I did have a student, perfectly healthy, apparently, who ended up in the hospital with covid last winter. Interesting that you only appear to be concerned about the health of the student portion of the “UO population.” I guess the 5000 staff don’t count in your book. I also know that from the fine graphs in the NYT, the median age of hospitalized covid patients currently appears to be right around 50. You seem to be a covid death cultist of the ilk of people like those guys at Stanford, the Harvard guy, the Great Barrington crowd. I think most people don’t want to follow. Even, these days, Donald Trump.
“You seem to be a covid death cultist of the ilk of people like those guys at Stanford, the Harvard guy, the Great Barrington crowd.”
I think it’s possible to question authority without immediately becoming a death cultist. In fact, science could scarcely even exist without those willing to question.
As far as death cultists go, though, here’s some data (ish) from the Illinois Department of Health. Scroll down to the “ICU Beds” graph. Apparently they’ve decided to let that number decline by 20-25% over the last 18 months. Unlike all of us here, someone there has actual power, and they made that happen. Or let it happen, if that’s a meaningful difference.
https://dph.illinois.gov/covid19/data/hospitalization-utilization.html
I think your anger is misplaced.
cruel irony duck: you consistently sound like a troll and not worth the time or energy for debate or discussion.
They do count. I’m one of them. I’m not a death cultist. But I’m a realist, and I’m an advocated for keeping schools open where ever possible, even though I initially was team shut the schools day in April of 2020.
But do you not think vaccination reduces hospitalization to “acceptable” risk levels, especially after being “boosted”? Do you deny “the science” around vaccination?
thedude: “But do you not think vaccination reduces hospitalization to “acceptable” risk levels, especially after being “boosted”?
No, vaccination alone is not enough and no, the United States is nowhere near an “acceptable” risk level even if you go by a fairly general risk assessment standard (see https://www.who.int/water_sanitation_health/dwq/iwachap10.pdf).
Vaccination is ONE mitigation (COVID19 requires the ‘swiss cheese’ approach: https://bmcinfectdis.biomedcentral.com/articles/10.1186/s12879-021-06357-4) but even if our country magically managed a 99% vaccination rate overnight, that would mean 3,320,000 humans would still be left to incubate and spread new mutations of the virus which may be unaffected by the vaccine. That magic scenario pretends the rest of the world doesn’t exist to make those numbers worse, of course.
However, our country’s “fully vaccinated” rate is a meager 62.4%. Oregon is a bit better at 68%. (ref https://www.mayoclinic.org/coronavirus-covid-19/vaccine-tracker). Worldwide the estimate is only at 59% (ref https://ourworldindata.org/covid-vaccinations)
That means even though you may be vaccinated and boosted, there’s a lot of folks who still aren’t. And that’s a problem which isn’t going to get resolved any time soon.
thedude: “Do you deny “the science” around vaccination?”
Only people who deny “the science” around science ask that question. Science is a process, not a conclusion. Assessments based on “the science” always have an asterisk attached; that invisible footnote reads “To the best of our knowledge at this date.”
Scientists are very careful to be exact with their language and acknowledge the limitations of their study when they provide their results. Unfortunately, too many people don’t get information directly from the scientists themselves (nor read the actual study writeup) and most are not familiar with known issues within any given specialty, which means there are frequently diverse misinterpretations by non-scientists when presented with the same “data” by journalists or politicians or PR teams from government agencies.
You say you’re a realist, so you should perhaps reflect on how hard you worked to specialize in whatever you are an expert on, then consider how much more work the vast majority of epidemiologists, virologists, immunologists, and related specialties have to put in to be considered an expert in their field… then LISTEN TO THEM CAREFULLY.
The experts seems split on this variant.
Many seem to concluding this well end the delta wave that was making it’s way through all the unvaccinated, perhaps at lower risk to the unvaccinated. It will do so much faster which could put strain on the health system. But most experts in the UK and other countries are nothing despite skyrocketing cases (because vaccines are not preventing infections, even among the vaccinated), they are not increasing ICU stays or deaths.
So I am listening to them carefully. But go ahead and type in all caps to make it seem like only you are.
Sorry for the caps, this format won’t allow italics for emphasis.
.
“Experts seem split on this variant” – who exactly (virologists? public health policy makers? economists?) are split on what about it (transmission rates? severity? likelihood of long-term sequelae?)? I haven’t heard any disputes over the basics (such as detailed in this article by Dr. Amir Khan https://www.aljazeera.com/features/2021/12/28/omicron-less-severe-but-still-dangerous)
.
You seem to be missing a few words in your post, so I’m guessing what you mean by “most experts in the UK and other countries are nothing despite skyrocketing cases is that they are “doing nothing”? Because that’s just flat-out incorrect. Heck, the UK government has updated its policy regularly: https://www.gov.uk/coronavirus and government officials aren’t even “experts”!
.
Worldwide, many people are WORRIED. For good reason. Other than China (https://www.science.org/content/article/china-s-aggressive-measures-have-slowed-coronavirus-they-may-not-work-other-countries), South Africa is the most hopeful, since their most recent wave (Omicron) peaked last month: https://www.bmj.com/content/376/bmj.o7 but the rest of the world is just now beginning or fully in the midst of our peaks (https://www.bbc.com/news/world-europe-59747689, https://ticotimes.net/2022/01/05/omicron-hits-hard-in-europe-us-and-latin-america).
.
It sounds like you are listening superficially, frankly. As if knowing the odds of an ICU visit or the likelihood of death is all that matters to you. If we were talking about, say, the H1N1 flu, that would be a perfectly reasonable position to take.
.
But even a truly mild case of COVID may leave damage (such as diffuse alveolar damage and thrombotic microangiopathy) that you might not even notice until down the road. And of course, we don’t have firm numbers yet how many folks are developing post-COVID myalgic encephalomyelitis (https://clinicaltrials.gov/ct2/show/NCT05059184).
.
Everyone – individuals, organizations, governments – should do as much as they possibly can to prevent the spread of this virus. That is what every respectable expert around the world has been saying. Claiming “well, this variant isn’t as lethal so let’s bring back chickenpox parties” (as many in these comments imply) is the opposite of what is needed.
.
This rant brought to you by a fully-vaccinated-and-boosted-yet-still-very-vulnerable member of your community.
This format does allow for italics
even, by magic
ITALICS
“But even a truly mild case of COVID may leave damage…” This is a real concern. I’d say a remote one, except that there’s so little credible data that there’s simply no way to tell.
Unfortunately, once one starts considering such things, one realizes that we’re in a rather similar state with respect to the vaccines themselves. Catastrophic long-term effects seem like a remote possibility, but again, there’s so little credible data that there’s simply no way to tell.
I’m rolling the dice, but not feeling very confident about my rationale.
(I will say, I’m noticing some changes in executive function since this all started. I’m sure it’s all in my head…)
204 more cases added for 1/5 as of this evening. The page is having some trouble loading.
Egads. The cases are changing like a one armed bandit.
10 pm update
the green bar is now at 404
the yellow bar is now at 84
Sure, but in logs it’s all fine.
I’m gonna go out on a limb here, but 500+ (and likely 750-1000 by 1/9) positive cases is NOT “very low”
throw in a factor of perhaps 5x for all the undetected infected students, and you’re up to maybe 5000. Virtually all the students after a month. No wonder it will be dropping like a stone soon. Hopefully before it gets to higher risk staff. Their rate looks to be 1/10 that of the students. Yikes. High enough to worry and low enough to keep trying. Not just the personal danger, but also disruption to classes. And I’m also concerned for all the unvaxxed. The attitude just to hell with the jackasses, I don’t like.
Today’s numbers are now 402/10ish/84
Egads – 638. Previous week 150ish, week before that 25ish. This coming week – 2000+?
Your lowly professor here reporting in sick. I began to fill out the UO reporting form and realized that those of us who are symptomatic and not feeling energetic enough to go stand in line for the hour or more it will take to get tested and then wait the several days to have our symptoms confirmed have no way to report transmission.
One of my classes is in a small classroom where distancing is impossible.
My family and I thank UO leadership for their foresight and planning.
If you can throw open the windows in one of those small classrooms, that will probably greatly reduce the covid risk. You don’t hear much about this from the authorities, for some reason.
When you posted the chart — on Wednesday? — this week’s infections were at 285. Today, Friday, they’re at 638. So much for all the messages about “We have confidence that …”
Do you think the administrators are waiting to declare all teaching will go online until the deadline for getting a full refund has passed? Or (even worse) will they just keep refusing and keep exposing everyone to infection, whatever the cost, in a 2022 version of the Charge of the Light Brigade?
The Knight Library is full of signs reminding patrons that masks are required. I think they probably should have worded that as “Masks are required to be *over nose and mouth* at all times”, given the number of masks worn ever-so-helpfully on the chin I saw today. At least this time no one swore at me when I reminded them…..
Tired of having the adults I ask to properly mask in my library launch into a tirade on the price of _(fill in the blank)_.